An Unusual Case of Hiccups
Case of persistant hiccups in a 91 year old man.

A 91 yr old man presented to an Urgent Care clinic with a four day history of frequent hiccups, occuring every few seconds. It was starting to affect his oral intake and I was concerned about his chances of responding to community treatment. He also looked Parkinsonian and I was thus concerned about using drugs such as chlorpromazine. I admitted him to the General Medicine team at the local hospital. He remained in hospital for over a week. He developed a moderate AKI. He underwent CT head/chest and abdomen which showed some minor abnormalities such as a hiatus hernia. OGD demonstrated a grade 3 oesophagitis. He was treated with a PPI and “low dose chlorpromazine”.
Learnings Nuggets1-5
- This is an uncommon presentation, and is probably only the second time I have seen this in my whole career.
- There are interesting definitions: Acute <48 hrs, Persistent= 48 hrs- 1 month, Intractable= > 1 month
- Persistent/intractable hiccup can have serious consequences- dehydration, malnutrition, sleep disturbance, exhaustion, depression, death has been reported.
- The actual physiology of hiccups is not clearly understood but is considered to be a reflex arc involving afferents(GABA/dopamine) from the phrenic nerve, vagal and sympathetics with efferents action via the phrenic. There is sudden contraction of the diaphragm and intercostals with sudden glottic closure (causes the "hic").
- Any pathology which potentially affects this pathway could cause hiccups.Gastro-oesophageal reflux is the most common cause of persistent and intractable hiccups but there are many potential serious causes which should be look for.
Causes:
Gastrointestinal- GORD,hiatus hernia,pancreatitis
Neurological- CVA(most common is lateral medullary syndrome),SOL,PD,MS
Malignancy-oesophageal,gastric, chest, neck, brain
Cardiovascular- ACS,pericarditis, thoracic aortic aneurysm/dissection
Respiratory- COPD/asthma, pleural effusion
Medications- ethanol, benzo's, azithromycin, dexamethasone, chemo, opiods
Metabolic- uraemia, hypocalcaemia, hypokalaemia, hyponatraemia
Psychological-fear, hyperventilation, air swallowing
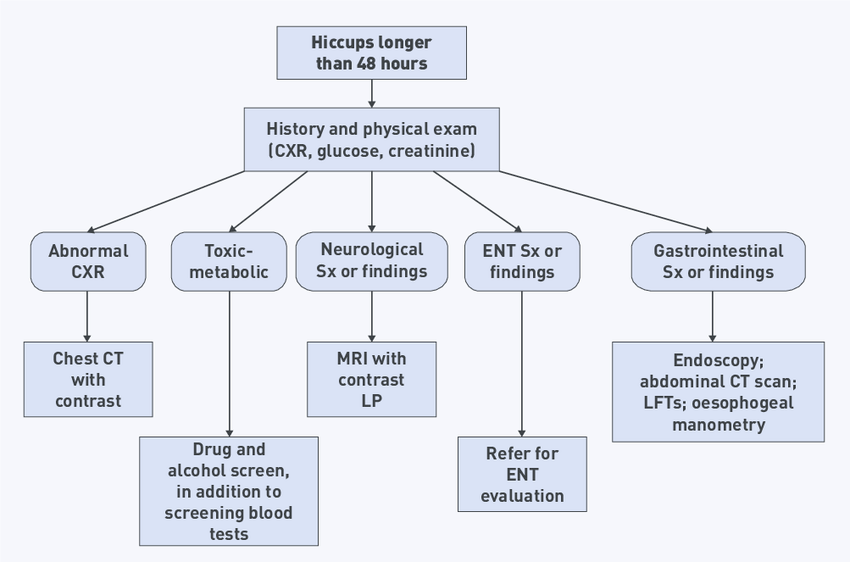
A suggested investigation algorithm:4
Management
- Most cases of persistent/intractable hiccups are likley to require hospital admission.
- Treat the underlying cause.
- Empirical use of PPI for GORD is sensible.
- If no treatable cause is found medication is indicated:1,3,5
Baclofen 5 mg TDS has been shown to be effective in several small randomized trials and observational studies is now considered the drug of choice for the treatment of hiccups.
Gabapentin 300 mg tds is an alternative.
Metoclopramide and chlorpromazine have been traditionally used but are limited by their extrapyramidal side effects.
A suggested management algorithm:5
References
- Cole JA, Plewa MC. Singultus. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025. Available: http://www.ncbi.nlm.nih.gov/books/NBK538225/
- Broadstock A. Taming the SRU. 2024. Diagnostics: intractable hiccups. Available from: https://www.tamingthesru.com/blog/diagnostics/intractable-hiccups
- Bhatti DMA, Sheikh AS, Fatima DM, Khan S, Groenewald DCA, Groenewald DES. Treatment approaches for persistent and intractable hiccups: a systematic review and recommendations. J Popl Ther Clin Pharmacol[Internet]. 2024 Mar 27;31(3):1757–67. Available: https://www.jptcp.com
- Quiroga JB, García JU, Guedes JB. Hiccups: a common problem with some unusual causes and cures. Br J Gen Pract [Internet]. 2016 Nov;66(652):584–6. Available: https://bjgp.org/lookup/doi/10.3399/bjgp16X687913
- Rajagopalan V, Sengupta D, Goyal K, Dube SK, Bindra A, Kedia S. Hiccups in neurocritical care. J Neurocrit Care[Internet]. 2021 Feb 1 ;14(1):18–28. Available: http://e-jnc.org/journal/view.php?doi=10.18700/jnc.200018



