Atraumatic back pain
A case of spinal cord compression in a 56 year old man. Discussion of learning points about clinical examination.

A 56-year-old man presented to urgent care with a six-month history of mid-thoracic back pain. He had no significant past medical history. A plain thoracic spine X-ray organised by his GP six months earlier had been reported as showing only degenerative changes.
Over the past three months his pain had progressively worsened, and he had developed bilateral lower-leg numbness and weakness. He described a burning sensation in both legs, as well as electric-shock pains precipitated by sneezing. Over the preceding week he had experienced increasing numbness in both legs, rising to the level of the costal margin. He rated his pain as severe (9/10). He denied bowel or urinary symptoms or erectile dysfunction. There was no history of fevers or weight loss.
On entering the consultation room I could see that he had an abnormal gait;slightly broad and high stepping. There was someting very wrong. Vital signs were normal. Chest and abdominal examinations were unremarkable. Upper-limb neurology was normal.
Lower limb neurological examination showed normal tone and power (5/5 in all muscle groups), reflexes were brisk bilaterally, with right ankle clonus, plantars were bilateral upgoing, there was a sensory level upto the level of the costal margin bilaterally, abdominal reflexes were present, anal tone was normal and Romberg’s test was positive.
Based on the examination findings, I diagnosed a thoracic spinal cord compression and referred him acutely to the orthopaedic team for emergency MRI.
MRI confirmed a large tumour mass at the T7 vertebral level involving the vertebral body and causing cord compression. Interestingly, his ESR and CRP were both normal. Subsequent biopsy established the diagnosis of a plasmacytoma/multiple myeloma.
This case reminded me of a patient I saw many years ago during my general medicine training days, when I was working as a gastroenterology senior house officer. The consultant had admitted a man in his sixties for further assessment after months of investigations for persistent right upper quadrant pain. Ultrasound, scopes, blood tests—all inconclusive.
I met him for the first time on a routine ward round with my house officer. We went over the now-familiar history of his abdominal discomfort, and then he casually mentioned an odd numbness in one leg. It seemed like a side issue, almost an afterthought, but something about it didn’t seem right.
I did a full neurological examination of his legs. He had brisk reflexes and clear ankle clonus—not really compatible with a simple hepatobiliary problem. In those days we didn’t have easy access to MRI scanning, so I discussed the case with one of the radiologists, who suggested a CT myelogram as the next best step.The myelogram was abnormal at multiple levels.
I referred him to the local neurosurgical unit, where he underwent an MRI. This confirmed spinal cord compression from tumour at several thoracic levels. The diagnosis had been missed because it was an unusual presentation and the consultant understandably had a skew in thinking towards his own speciality.
Of course, this did not win me any favours with my consultant! But it taught me a lesson I’ve carried throughout my career: sometimes the answer to a grey case lies just outside the frame you’ve been given. One stray comment, one unexpected sign, one decision to examine a bit more broadly—and the whole picture can change.
Learning Nuggets
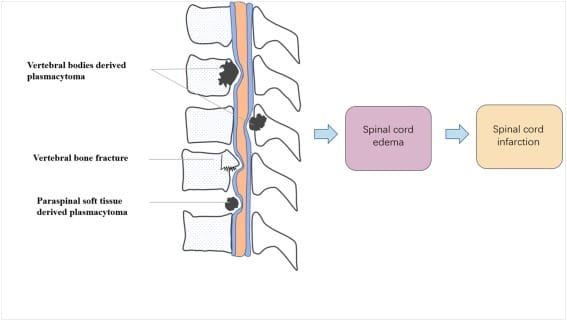
*Spinal cord compression (SCC) in multiple myeloma(MM) can be caused by vertebral bone-derived plasmacytoma, vertebral bone fracture, and paraspinal soft tissue-derived plasmacytoma. Spinal cord edema and infarction will develop eventually with loss of neurological function. It is an emergency.
*Approximately 70 % cases SCC in multiple myeloma are thoracic. SCC occurs earlier in MM than with other solid tumours and can be the presenting process.
*Approximately 35 % of patients present with motor deficits at the time of diagnosis. Isolated/painless ataxia can be the presenting symptom. Bladder and bowel disturbance are late signs. The spinal sensory level is usually 1-5 segments below the level of cord compression. There can be significant variability in the clinical signs.
*MRI is the first line investigation for suspected SCC but CT myelography still remains a valid alternative for patients who cannot undergo MRI.
*Acute SCC is a medical emergency and treatment should be started within 24 hours of diagnosis.
Bone is the third most common site of metastasis after the liver and lung.
*High Index of suspicion for metastatic SCC: known cancer diagnosis, night time pain when moving, bilateral nerve root pain/radiculopathy, unsteady gait, progressive limb weakness, bowel/bladder dysfunction.
*Plain XR is often performed but is a poor test for spinal metastasis and will only pick up those cases with vertebral collapse/pathological fractures.
Onset of SCC
*insidious onset over months or
*acute eg destructive vertebral collapse, rapidly developing epidural abcess
In my experience the clinical signs of SCC are often not "classic". They can be subtle, variable and asymmetrical. The key is to know the classical signs and maintain a high index of suspicion in at risk groups or those with red flags.
With the first patient I knew there was a problem just by observing his gait but it was difficult to precisely classify gait disturbance. I have not seen a precise definition of a classic "SCC gait" although there is a "myelopathic gait" used is association with cervical myelopathy often described as a wide-based, spastic gait. With this patient it seemed more like a sensory ataxic gait. The appearance of the gait in SCC will logically depend on the site, severity and degree of evolution.(See the Standford gait disorder video below)
Clinical Signs of Spinal Cord Compression
Gait disturbance-myelopathic
Weakness most apparent in proximal muscles of legs
Band-like hyperesthesia initially around trunk at level of compression progressing to anaestheia below this level
Romberg's test positive.
LMN signs at level of lesion and UMN signs below.
Classic spastic paraparesis:
- increased tone
- weak
- bilateral hyperreflexia
- bilateral ankle and patella clonus
- bilateral extensor plantars
- loss of abdominal reflexes
- sensory level
Differential of spastic paraparesis:
- Cord compression
- MS
- Trauma
- Birth injury
- MND
- Rare- Subacute combined degenneration cord, transverse myelitis,parasagittal meningioma, anterior spinal artery thrombosis, taboparesis, Friedreich's ataxia, HIV/AIDS myelopathy
Further Reading
- Chen B, Cai L, Zhou F. Management of acute spinal cord compression in multiple myeloma. Crit Rev Oncol Hematol [Internet]. 2021 Apr 1;160:103205. Available from:https://www.sciencedirect.com/science/article/pii/S1040842820303413
- Nair C, Panikkar S, Ray A. How not to miss metastatic spinal cord compression. Br J Gen Pract [Internet]. 2014 Sep;64(626):e596–8. Available from:https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4141619/




