Beware Flank Pain

I was working at an Urgent Care facility in a ski resort one weekend during the ski season. A man in his 60's came in complaining of significant L flank pain. He had been skiing with his wife and had developed the pain just as they were finishing for the day. There was no history of any fall or incident when skiing. He came straight to the clinic from the mountain. He had a history of hypertension for which he took metoprolol. There was no history of renal stones. His blood pressure was normal. His abdominal exam was unremarkable, no palpable AAA, and there was no flank tenderness. Auscultation of the heart and chest were also normal. There were no pulse deficits or signs of limb ischaemia and no overt neurological signs. I performed a 12-lead ECG which just showed a mild sinus bradycardia which was consistent with beta-blockade.
He was clearly in a lot of pain. He was very restless, pacing around then lying down then standing up. He could not get comfortable. There was no diaphoresis or signs of shock. My initial thought when he first came in was that he had some form of back injury. During the ski season we would see large numbers of patients with all manner of skifield injuries. There was no radiation of the pain and the presentation somehow did not have the feel of renal colic. After assessing him though my instinct was telling me that there was something not quite right here. His restlessness was concerning and his degree of pain seemed inconsistent with the clinical findings. I was starting to think about serious diagnoses such as aortic dissection(AD) but there did not seem to be enough clinical features to support the diagnosis. He only had flank pain. I wanted to do a CXR to look at his mediastinum but by chance our radiology unit was closed. I had no point of care ultrasound(POCUS). I decided to give him some analgesia and decide what to do.
The only option for referral locally was to a rural hospital with no CT capability, the nearest base hospital being 2 hours away by road. A few minutes after taking the analgesia he vomited. This is not right I thought, he needs to be admitted and have a CT chest and abdomen. I referred him to the duty doctor at the local rural hospital as per our usual procedure. Any transfer to a bigger center would be arranged from there. I explained my concerns and raised the possibility of aortic dissection.
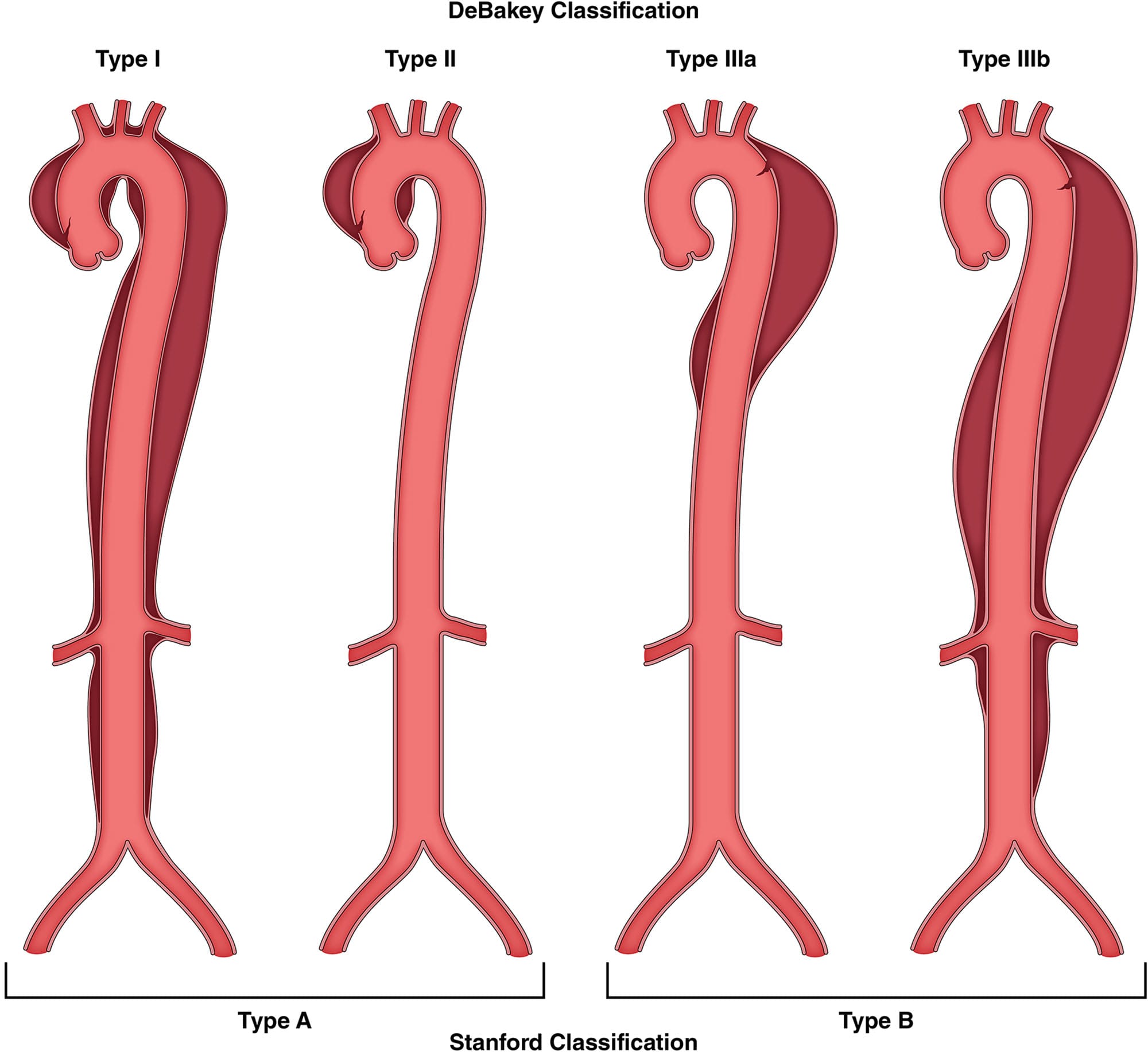
The rural hospital doctor performed a CXR which showed a normal mediastinum. He was admitted to the ward at the hospital and given intravenous opiates. I am not aware of the decision making at this stage but he was not transferred to a regional referral hospital. Some hours later he arrested and died on the ward. A post mortem examination showed a large Stanford Type A aortic dissection. The attending doctor was distraught and needed collegial support.
I have wanted to discuss this patient for a long time now. I want to raise awareness about AD because this is an area of medicine where there is clear potential for saving lives.
I also want to raise awareness about the diagnosis of flank pain. If I hear mention of "flank pain" at work I am immediately on high alert. There are so many differentials which are easy to miss yet all the time I find this is under recognised. This is a topic I will come back to in future posts.
During my career I have seen several aortic dissections and in a future post I will document some of these. I would be keen to hear from readers about any aortic dissection cases you have been involved with. We could potentially make a repository for reference and teaching.
Learning Nuggets
- Always beware of flank pain. Anyone who works with me knows this is my mantra. There are so many potential causes of flank pain and over the years I have seen many misdiagnoses.
- The Aortic Dissection Charitable Trust UK estimates that 33 % of cases of AD are misdiagnosed and 10 lives per week could be saved with the correct diagnosis. About 50 % of people with a Type A dissection die before hospital arrival. If they survive to hospital their mortality increases by 1% per hour, reaching 50% at 48 hours. With prompt diagnosis and treatment though the operative survival for Type A dissections is about 80%. The Trust is doing great work to raise awareness about AD and save lives.1 Check out the resources on their website (https://aorticdissectioncharitabletrust.org/healthcare-professional-resources/)
- 70% of dissections are Stanford Type A.1
- There is no typical presentation of an aortic dissection and it is often misdiagnosed. They may be asymptomatic on presentation or have a complex mix of symptoms from different organ systems.1 About 10 % of patients have no pain.3 Clinicians need to have a clear understanding of the limitations of clinical assessment.
- Flank pain is probably an under recognised presentation of acute AD which is thought to be due to eithet renal ischaemia, renal capsule stretching, retroperitoneal irritation or referred pain from shared visceral afferents. Beware flank pain!
- Red flags: age 50-65 (75 % cases), PMH hypertension(most important risk factor), pain maximal at onset then improving (compared to crescendo pain in ACS), chest or back pain plus symptoms/signs related to different organ symptoms, genetic disorders (e.g Marfan's, vascular Ehlers-Danlos), pregnancy.2,3,4
- AD should be considered in any "strange" clinical scenario where things do not add up, particularly when there are symptoms or signs in 2 or more organ systems. We should also consider it and look for signs when patients present with other more common problems e.g seizures, CVA, TIA, collapse, abdominal/flank pain.
- Consider it. Diagnose it. Exclude it.1 The only way to reliably exclude it is with a CT scan.1 A normal CXR does not exclude it ("normal" in up to 20%, widened mediastinum in only 50-60%).2,3,4 Blood pressure discrepancies between the upper extremities, pulse deficits, or a diastolic murmur of acute aortic regurgitation are found in less than 50%.3 A normal ECG does not exclude it- MI due to involvement of coronary arteries is rare.3
- Symptoms are the key with considering AD. A 2024 report from the HDC documents a case of missed AD in a 70 year old lady who presented twice in two days to her local ED and then died. The initial symptoms were chest pain, shortness of breath and collapse.5
- Restlessness or pain severity inconsistent with clinical findings is always a red flag.
- Poorly controlled pain is always a red flag and should trigger a review of the diagnosis.
- POCUS , if available, can quickly identify a pericardial effusion and signs of tamponade=game changer for the urgent care physician.
Further Reading
- Aortic Dissection Charitable Trust. Aortic Dissection Charitable Trust. Available from: https://aorticdissectioncharitabletrust.org/
- Rogers J, Hayes J, Hayes JR. Acute aortic dissection. Life in the Fast Lane (LITFL). Available from: https://litfl.com/acute-aortic-dissection-ffs/
- Levy D, Sharma S, Farci F, Le JK. Aortic dissection. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2026. Available from: http://www.ncbi.nlm.nih.gov/books/NBK441963/
- Isselbacher EM, Preventza O, Black JH. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease. Circulation. 2022 Dec 13;146(24). Available from: https://www.ahajournals.org/doi/10.1161/CIR.0000000000001106
- Health and Disability Commissioner. Diagnosis of aortic dissection. Available from: https://www.hdc.org.nz/decisions/search-decisions/2024/22hdc01091/



