Bradycardia and syncope
Case of bradycardia and possible BRASH syndrome in a 70 year old man.

A 70-year-old man presented to urgent care after two sudden collapses that day, associated with brief loss of consciousness. His past medical history included hypertension and type 2 diabetes. He had no previous cardiac history. Medications included felodipine, losartan, metformin, empagliflozin and Lantus. He had been well the last few days and had not missed any doses of medications.
On examination he was alert, looked well, and was even making jokes. He looked hydrated. His heart sounds were normal, chest clear, and blood pressure was 110/65 mmHg. He had warm and well perfused peripheries. BSL was 23 and ketones 0.5.
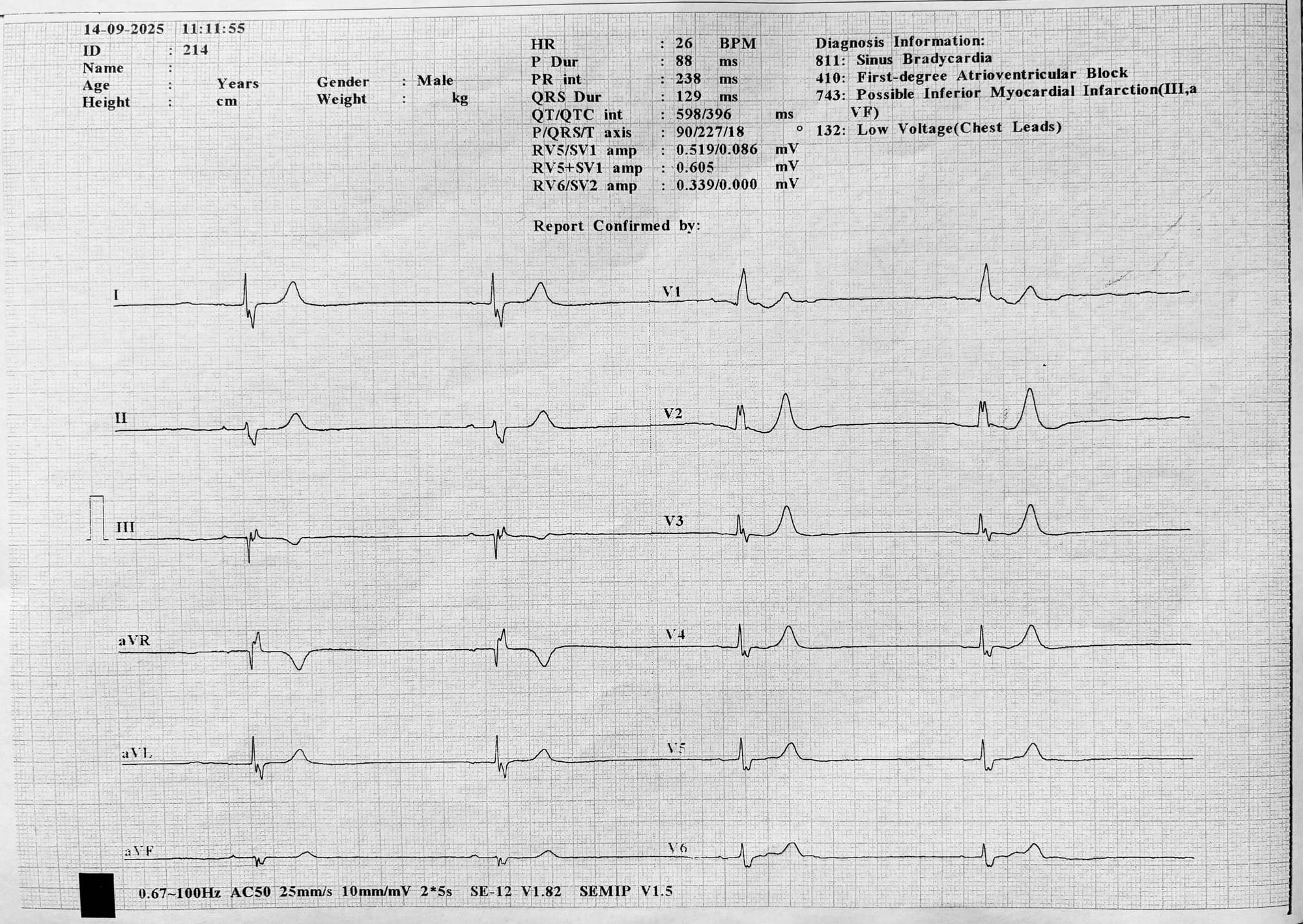
ECG findings: Sinus bradycardia with a ventricular rate of 26 bpm, First-degree AV block, Right bundle branch block, Leftward axis, No signs of STEMI, possible tenting of T waves.
I called a P1 ambulance and gave him 600 µg of atropine IV. There was no effect his heart rate dropped lower to 22 bpm, though he remained surprisingly well.
Time for a second-line agent. Our clinic does not stock isoprenaline, so adrenaline was the only option. I used a "dirty-adrenaline infusion". His heart rate improved to between 30–40 bpm by the time paramedics arrived, and he was transported to the emergency department.
In ED, the adrenaline was stopped and an isoprenaline infusion commenced. Blood tests showed several abnormalities: K+6.6, Na +132, Ur 14.4, Cr 147, pH 7.37, HCO3- 23, AG 11, lactate 3.2, ketones 0.5.
He was admitted to CCU, where echocardiography demonstrated normal left ventricular size and function, with evidence of mitral stenosis and sinus bradycardia at 40–50 bpm. It is uncertain if he had any other interventions at this stage but the patient possibly remembers having some IV fluid and his usual insulin. Repeat bloods 3.5 hours later showed a normal K +5.0.
The following day, he underwent permanent pacemaker insertion and was discharged home the day after that.
Learning Nuggets
*Severe bradycardia is an infrequent occurence in Urgent Care but it is one of those peri-arrest situations where we might need to take action before paramedics arrive. As always preparation and rehearsal are key.
*Algorithms provide good frameworks and mental models for teams but we have to be aware of their limitations. They often don't cover all the nuances of peri-arrest situations or give explicit intsructions. Failure to understand this can lead to overconfidence and then confusion when faced with a messy real situation.You need more knowledge to really master the situation.
*I wont discuss the deranged blood chemistry here but I think he may have had BRASH syndrome (Bradycardia, Renal failure, AV node blockade, Shock, Hypotension).2 There is alot to discuss here so I will come back to this in a later post.
*A four-step approach2 can be used to supplement the algorithm. These represent a diagnostic process,running simultaneously.
1. Is this patient stable or unstable?
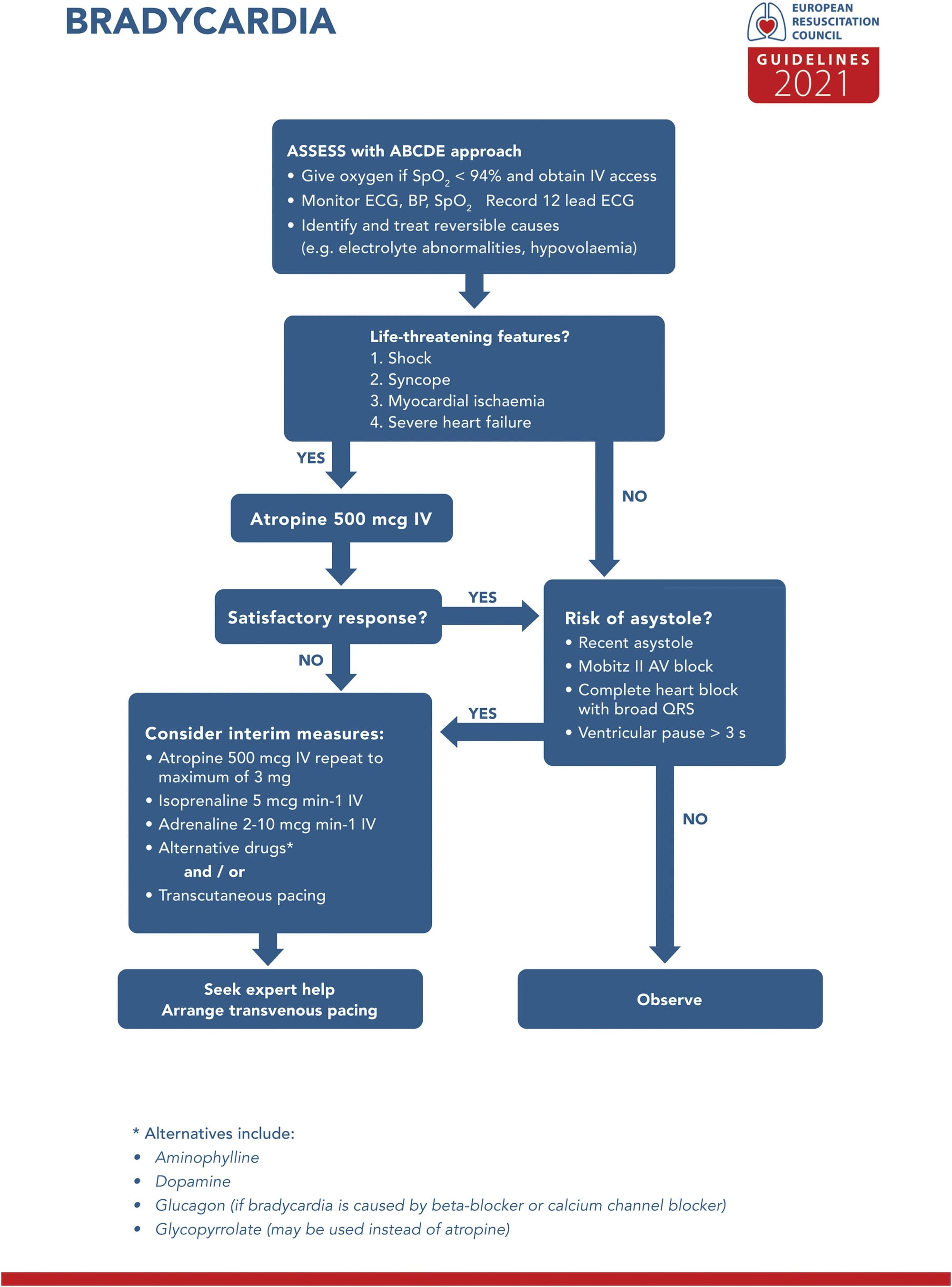
This is the first and most important question, as it determines whether immediate emergency drugs need to be given.This is essentially the "Life Threatening Features" box.1 At first glance, the patient looked stable; he was alert, cheerful, joking about the rugby, and had a seemingly adequate blood pressure. However, he was not stable. He had already experienced two syncopal episodes — a life-threatening feature in the ERC bradycardia guideline.1 These episodes may have been caused by ventricular pauses, which carry a risk of progression to asystole. This was not a bradycardic periarrest sitaution but he was still on a knife edge.
With well looking, normotensive patients we need to be cautious about normotensive(occult) bradycardic shock where the BP is being maintained by a vasoconstrictor response. This is still a low cardiac output state and thus makes the patient unstable. He was warm, well perfused, and had normal mentation. With a HR in the 20's in a 70 year old man with prior hypertension his cardiac output must be reduced. His admission bloods would tend to suggest some renal hypoperfusion.
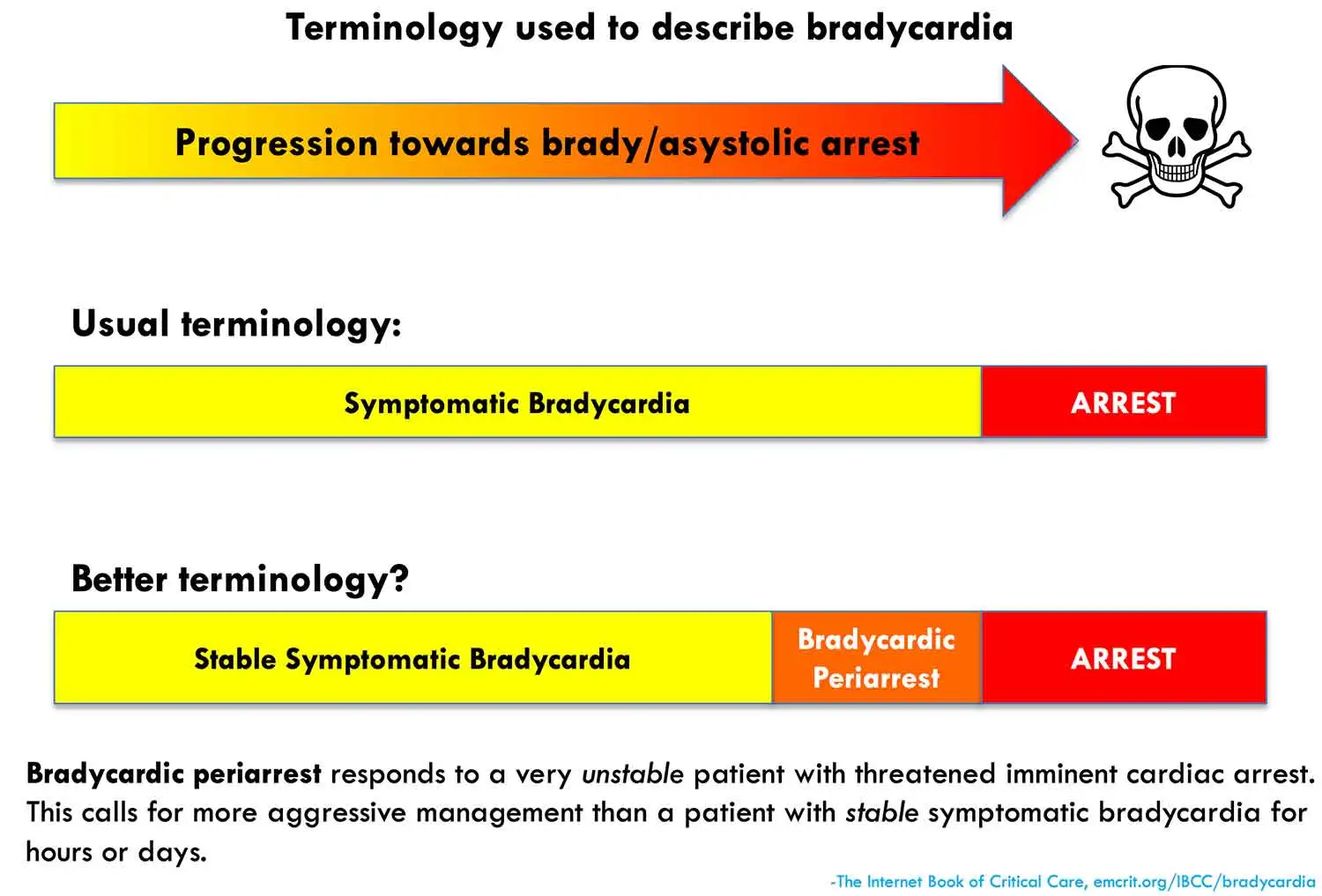
A change in terminology is useful, courtesy of EMCrit blog.5
2. Is the patient symptomatic or asymptomatic?
Is it the bradycardia causing the symptoms or is it some pathology causing the bradycardia? If a patient with bradycardia is stable and asymptomatic, immediate treatment is not usually required. He was symptomatic, as evidenced by syncope. There was no history of chest pain or symptoms of DKA;important considerations given his diabetes.
3. Where is the likely anatomical site of the bradycardia? Sinus node dysfunction or AV block?
This will affect the response to medication and help predict the need for permanent pacing. A narrow complex QRS will tend to indicate a proximal block in the SA or AV node. A wide complex QRS(>120ms) can represent proximal or distal block ("south" of AV node or infranodal). Distal disease in the His-Purkinje system doesnt respond to medications and usally requires pacing.
The ECG showed: RBBB pattern, Leftward axis, First-degree heart block.
Traditionally, this combination is referred to as trifascicular block, which can progress to complete (third-degree) heart block. He clearly had significant conduction system disease which may have been present for some time.
4. Are there any secondary causes of bradycardia?
Secondary causes (occurring outside the conduction system) are common (80% cases) and should always be considered.
-The history of diabetes should raise concern about cardiac ischaemia.Bradycardia and diabetes should always raise the concern about possible DKA and hyperkalemia. He was compliant with his meds.
Bradycardia Mnemonics:
4 most common life threatening causes= KIDI
K-hyperkalaemia
I-ischaemia
D-drugs
I-increased ICP
Causes= DIES
-Drugs – beta blockers, digoxin,CCB
-Ischaemia / Increased ICP
-Electrolytes(K+, Environmental(hypothermia), Endocrine(myxoedema)
-Structural heart disease, Sepsis, Saturation(hypoxia), Surgical(paradoxical)
NB in a renal dialysis patient presenting with bradycardia the most likley diagnois would be hyperkalaemia and immediate management of this, even before a K+ level is available, would be appropriate starting with calcium gluconate.This is a common scenario in EDs when pateints have missed their dialysis.
NB A paradoxical bardycardia from a vagal response is sometimes seen with a ruptured abdominal viscus,ectopic pregnancy or haemorrhagic shock.3
NB Cardiac arrest in children is usually a brady-asystolic progression often due to hypoxia. Oxygenation and ventilation are key interventions.
When is atropine useful?1,4,5,6
Atropine is the recommended first-line agent but overall only about 28% of patients respond6 so basically don’t delay escalation if there’s no effect.
-Dose: 500–600 µg IV bolus. Repeated doses every 3–5 minutes up to a total dose of 3 mg are recommened.1,4,6 I have never seen this done in practice and my concern here is that it delays starting second line agents.
-Atropine is ineffective in cardiac transplant patients (denervated heart won’t respond to vagal blockade, and it may paradoxically worsen AV block).
-Works best for sinus bradycardia, junctional bradycardia, and proximal AV block (within the AV node) e.g inferior MI
-Rarely effective in distal AV block (Mobitz II, third-degree block, idioventricular rhythms).
What is the best second-line agent?4-7
In New Zealand, the two most commonly used agents are isoprenaline and adrenaline.
-Adrenaline (epinephrine) – recommended by ANZCOR as the second-line agent at 2–10 µg/min titrated to effect. It increases heart rate and contractility, and its alpha effect provides vasoconstriction, which is useful if hypotension or cardiovascular collapse is present.
-Isoprenaline (isoproterenol) – commonly used in NZ emergency departments but rarely available in urgent care. More selectively chronotropic (increases rate without strong alpha effects), but may cause vasodilation and hypotension. Evidence supports its use in third-degree AV block.7
-There are no RCTs comparing adrenaline vs isoprenaline. The choice should be individualised: adrenaline if hypotension/shock is present; isoprenaline if unstable AV block with preserved blood pressure.
Indications for transcutaneous temporary pacing?1
This is another option but not widely available in NZ urgent care.
Indications mirror the risk factors for asystole in the ERC bradycardia algorithm.1
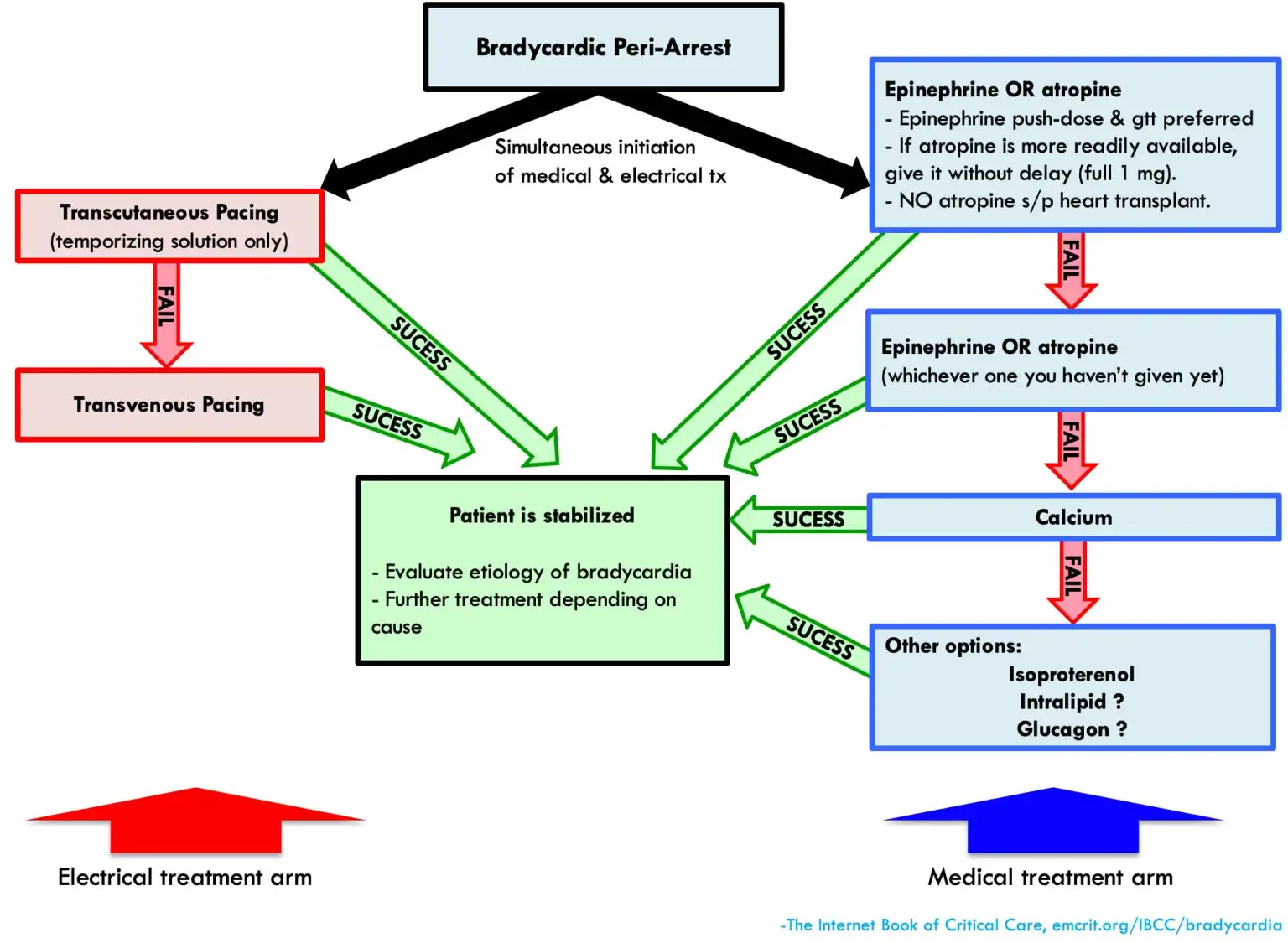
Management of bradycardic peri-arrest?5,6
If there is severe bradycardia with shock or rapidly worsening bradycardia("bradying down") over seconds to minutes this is a peri-arrest situation.
-Give push-dose adrenaline 10–20 µg IV adrenaline stat
-Set up transcutaneous pacing if available.
-Prepare and commence an adrenaline infusion.
-If hyperkalaemia is suspected start treating this.
-A suggested algorithm by EMCrit.5
How do you make up push-dose adrenaline?5,6
-Take 1 mL of 1:10,000 adrenaline (100 µg).
-Dilute with 9 mL of normal saline in a 10 mL syringe.
-This gives a concentration of 10 µg/mL.
What is the easiest way to make up an adrenaline infusion in Urgent Care?5,6
The simplest method is the “dirty adrenaline infusion”:
-Add 1 mL of 1:1000 adrenaline (1 mg) to 1000 mL of normal saline.
-This gives 1 mcg/ml
-Start the infusion slowly and titrate to response.
-This is fine via a peripheral IV
References
- European Resuscitation Council. ERC guidelines [Internet]. 2021. Available from: https://cprguidelines.eu/guidelines-2021
- Emergency Medicine Cases. 4-step approach to bradycardia and bradydysrhythmias [Internet]. Available from: https://emergencymedicinecases.com/approach-bradycardia-bradydysrhythmias/
- Bell K, Elmograbi A, Smith A, Kaur J. Paradoxical bradycardia and hemorrhagic shock. Proc (Bayl Univ Med Cent) [Internet]. 2019 Mar 14;32(2):240–1. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6541057/
- Australian and New Zealand Committee on Resuscitation (ANZCOR). Guideline 11.9 – Managing acute dysrhythmias [Internet]. Available from: https://www.anzcor.org/home/adult-advanced-life-support/guideline-11-9-managing-acute-dysrhythmias
- EMCrit Project. Bradycardia [Internet]. Available from: https://emcrit.org/ibcc/bradycardia/
- Emergency Medicine Cases. Treatment of bradycardia and bradydysrhythmias [Internet]. Available from: https://emergencymedicinecases.com/treatment-bradycardia-bradydysrhythmias/
- De Lazzari M, Martini N, Migliore F, Donato F, Babuin L, Tarantini G, et al. Efficacy and safety of isoprenaline during unstable third-degree atrioventricular block. J Cardiovasc Dev Dis [Internet]. 2023 Nov 25;10(12):475. Available from: https://www.mdpi.com/2308-3425/10/12/475



