BRASH syndrome
Case of BRASH syndrome

Last week I discussed the case of a 70 year old man presenting with syncope and bradycardia. If we take a deep dive into this case you will see many learning points. It was difficult to establish all the facts because the discharge paperwork from the hospital was limited so this is just my surmising.
Firstly you may remember that the patient had very deranged blood chemistry on arrival at hospital: K+6.6, Na+132, Ur 14.4, Cr 147, pH 7.37, HCO3-23, Anion Gap 11, lactate 3.2, ketones 0.5, HbA1c 101, ACR 44.5.
Interpretation:
Hyperglycaemia (23.8) – suggests uncontrolled diabetes, but this is not DKA (pH, bicarb and AG are normal). The calculated serum osmolality is 301 mmol/kg which is slightly elevated but still below the diagnostic criteria (320) for hyperosmolar hyperglycaemic state (HHS). This glucose level could also be partly due to a stress response and the adrenaline infusion.
Severe hyperkalaemia (K⁺6.6) — the key and most dangerous abnormality, causing suppression of SA and AV node conduction and potentiating the effect of any pre-existing conduction system disease. The patient was on felodipine but this is a dihydropyridine calcium channel blocker (CCB) and does not directly depress AV nodal conduction; it will cause perpheral vasodilation and in patients with severe bradycardia or hypotension, it could indirectly worsen renal perfusion.
Mild hyponatraemia- this is likley a dilutional effect of the hypergylcaemia.
Renal impairment (urea/creatinine elevated) — this is likely from dehydration, ARB inhibitor use, underlying diabetic nephropathy and acute renal hypoperfusion leading to reduced clearance of potassium and metformin.
Mildly elevated lactate — likely adrenaline-related and/or due to poor perfusion during bradycardia. This is not a lactic acidosis.
Microalbuminuria + elevated HbA1c — chronic diabetic nephropathy background.
I dont know the exact details of the management in hospital particularly with regard to hyperkalaemia but the K+ had normalised 3 hours later. Better renal perfusion with fluids and adrenaline/isoprenaline would have helped this with the latter two agents also tending to drive K+ into cells (beta-2 stimulation). The following day his glucose had normalized and he underwent insertion of a permanent pacemaker. I dont know if BRASH syndrome was even considered. On reflection I suspect there were a combination of things going on. He probably had some longstanding significant conduction system disease which was made worse with some degree of BRASH.
In summary the patient has severe hyperglycaemia with mild hyperosmolality, but does not meet diagnostic criteria for HHS. He has non-ketotic hyperglycaemia due to poorly controlled diabetes, complicated by AKI, hyperkalaemia, and BRASH physiology.
BRASH syndrome — an acronym for Bradycardia, Renal failure, AV nodal blockade, Shock, and Hyperkalemia — was first formally described by Josh Farkas in 2016 on the PulmCrit blog, part of the EMCrit Project.1 The syndrome is essentially a viscious cycle which develops from hyperkalaemia, renal failure and medications. Hyperkalaemia and AV nodal blocking drugs act together to produce bardycardia.
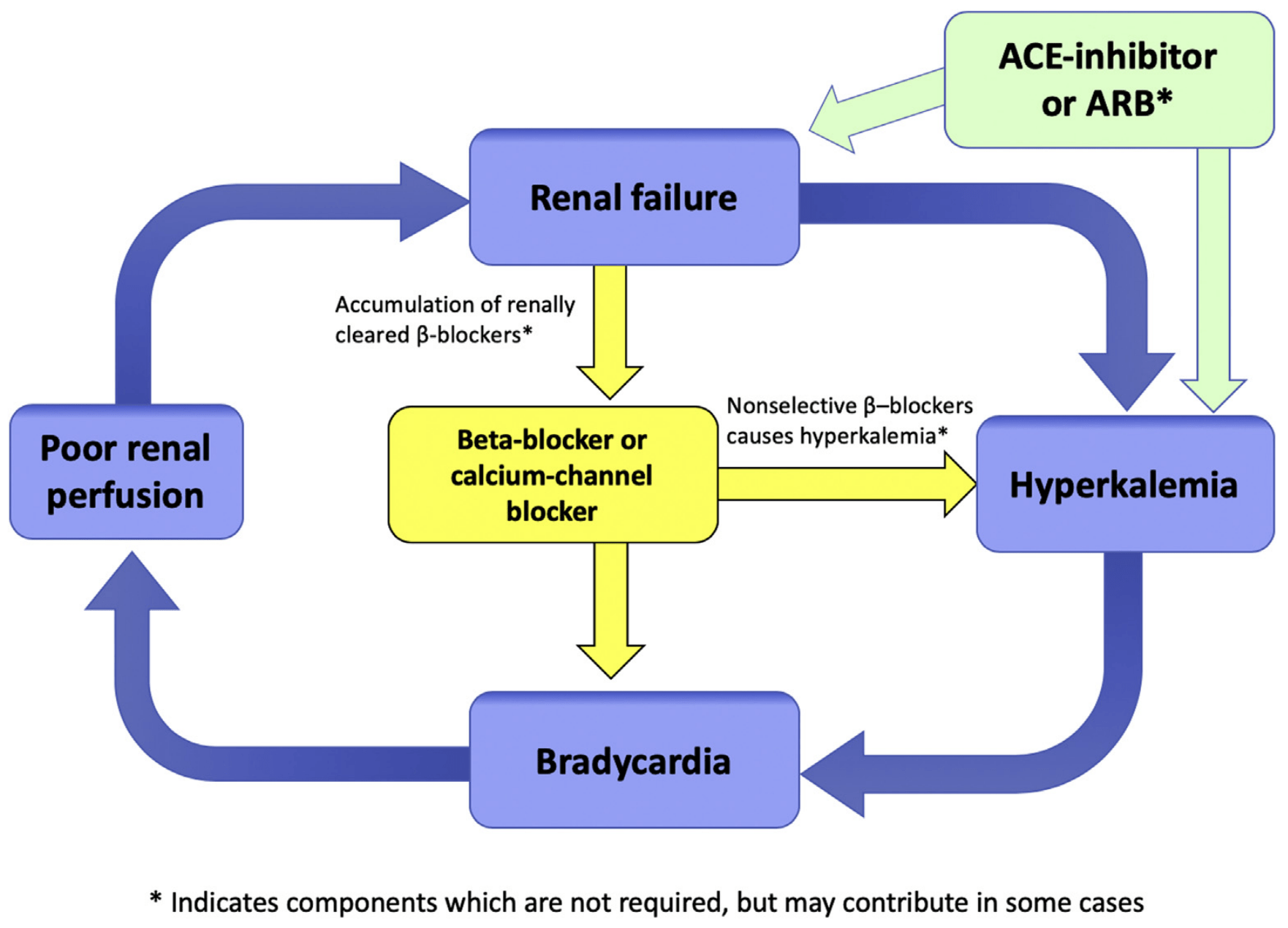
Courtesy Farkas/PulmCrit.1,2
The syndrome is an overlap of hyperkalaemia and AVN blocking drug excess.
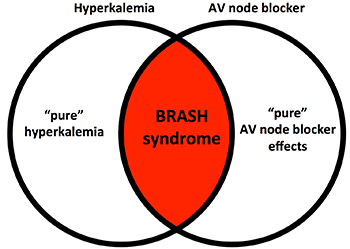
*Courtesy of Farkas/PulmCrit.1
BRASH is most common in elderly people with reduced renal reserve on multiple medications. It is commonly triggred by any cause of hypovolaemia such as gastroenteritis or a dosage increase of medication.
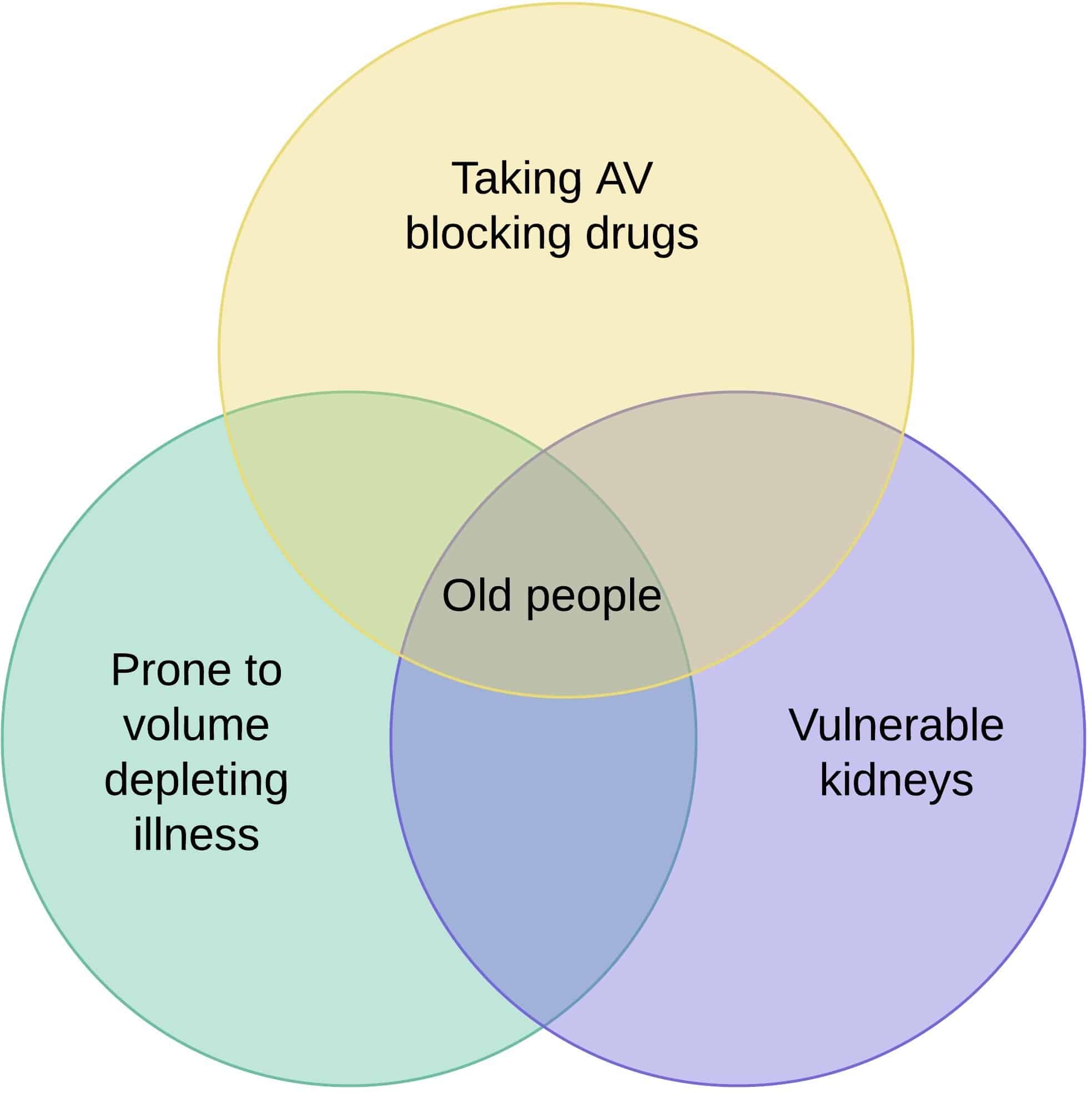
*Courtesy of LITFL3
The clinical presentation can be broad ranging from mild bradycardia to shock and multiorgan failure.
The priorities of management are:1
1/ Hyperkalaemia- iv calcium, iv insulin/dextrose. Dialysis may be required in severe cases.
2/ Fluid resuscitation-NB the volume status in these patients apparently varies widely but dehydration from gastroenetritis is a common precipitant.
3/Catecholamine infuison- To support perfusion and heart rate. NB Patients may have occult bradycardic shock where the degree of renal hypoperfusion is not appreciated because vasoconstriction is maintaing a "normal" BP. Their cardiac output will still be low because after a certain point stroke volume will not be able to compensate for bradycardia.
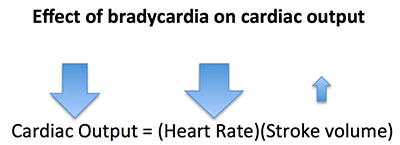
Courtesy of Farkas/Pulmcrit.1
Isoprenaline is the drug most commonly used for bradycardia in emergency departments in NZ.Its advantage is that it can be used peripherally due to its vasodilator properties.Its disadvantage is that can potentailly lower BP/MAP because of this peripheral vasodilation since it has no alpha effects.In this patient this would be more of a concern because of his mitral stenosis. Adrenaline is probably better for shocked patients and will reduce potassium more than isoprenaline.
BRASH syndrome is probably under recognized by all frontline specialities. In the future I can see that urgent care clinics may have access to more point-of-care testing such as venous blood gas which may enable us to diagnose hyperkalaemia quicker. This would hopefully trigger consideration of BRASH. It is also good for us to understand the vulnerability, especially of elderly people to this syndrome and to be on the look out for it.
Take home point: In older people with bradycardia think BRASH
References
- Farkas J. PulmCrit – BRASH syndrome: bradycardia, renal failure, AV blocker, shock, hyperkalemia. EMCrit Project [Internet]. 2016.
- Farkas JD, Long B, Koyfman A, Menson K. Brash syndrome: bradycardia, renal failure, AV blockade, shock, and hyperkalemia. J Emerg Med. 2020 Aug;59(2):216–23. https://doi.org/10.1016/j.jemermed.2020.05.001
- Cassidy T, Cadogan M, Cadogan TC. BRASH syndrome. Life in the Fast Lane (LITFL) [Internet]. 2021.
- Lizyness K, Dewald O. BRASH syndrome. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025.



