Chest pain in a 45 year old woman.
Case of an SCAD presenting in a 45 year old woman. Discussion of important aspects including hyperacute T waves on ECG and management of RV infarction.

A 45-year-old New Zealand European woman presented to urgent care after a two-hour episode of severe central chest pain. The pain was tight, non-radiating, and associated with a general feeling of being unwell. She denied shortness of breath. She had no significant past medical history, no family history of ischaemic heart disease, did not smoke, and was not on oestrogen therapy.
On examination, she appeared distressed but not diaphoretic. Her pulse was 80 and regular. Her blood pressure was borderline at 95/70. Heart sounds were normal and her chest was clear. She was warm peripherally and her mentation was normal.
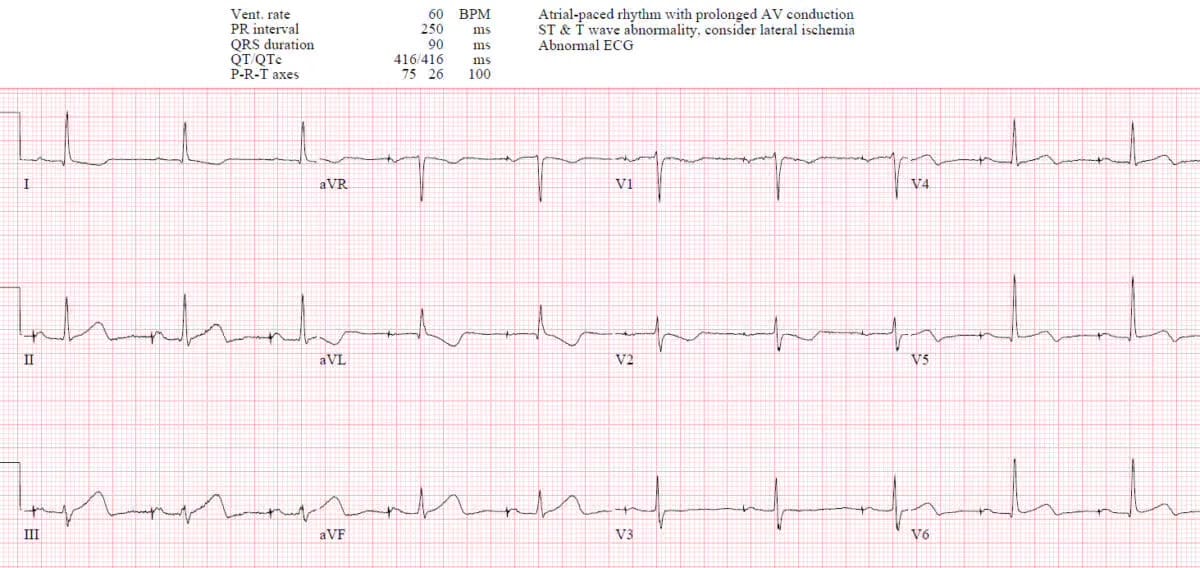
The ECG showed hyperacute T waves in the inferior leads (II, III, aVF) without reciprocal changes. I diagnosed a possible early inferior STEMI and immediately called a 111 ambulance. Because of her hypotension and the inferior changes I suspected a right ventricular infarct and gave 500 mL of normal saline.I gave IV fentanyl 20 mcg for pain in view of the potential haemodynamic instability.
When the paramedic crew arrived, they were dismissive of the ECG changes and felt there was nothing to worry about! My heart sank. I explained the ECG changes and politely asked that they transport the patient to hospital immediately and not wait for a referral letter! I phoned the cardiology registrar at the regional referral centre to activate the STEMI pathway, but he declined and advised sending the patient to ED. I then spoke with the ED consultant, who was also initially uninterested.
On arrival, the attending ED consultant agreed with my diagnois of hyperacute T-wave changes, and the STEMI pathway was activated. The patient underwent coronary angiography and was found to have a spontaneous coronary artery dissection (SCAD), from which she later recovered well.
Learning Nuggets
- SCAD is an under-diagnosed condition. The diagnosis is often missed and there is a lack of familiarity with the condition amongst doctors. There is low suspicion in young women without risk factors even in the context of classic ACS type symptoms.1,2 There is an urgent need for greater awareness about SCAD. The key thing is to know the classic demographic and consider the diagnosis.
- The true prevalence of SCAD is uncertain. The vast majority of cases are in women(90%). SCAD may be the cause of up to 1 - 4% of ACS cases. Possible cause of upto 35 % MI in women<50 and is most common cause of MI in pregnancy (43%).1,2
- The etiopathogenesis not fully understood. The main risks factors are female sex, pregnancy, and physical and emotional stress triggers; and concurrent systemic arteriopathies, particularly fibromuscular dysplasia and inherited conditions e.g vascular Ehlers Danlos.1
- The classic demographic for SCAD is the european woman age 45-53 without any risk factors for atherosclerosis. Cases have occured in women in their 20's. In pregnancy related cases, most occur in first 4weeks postpartum.1,2
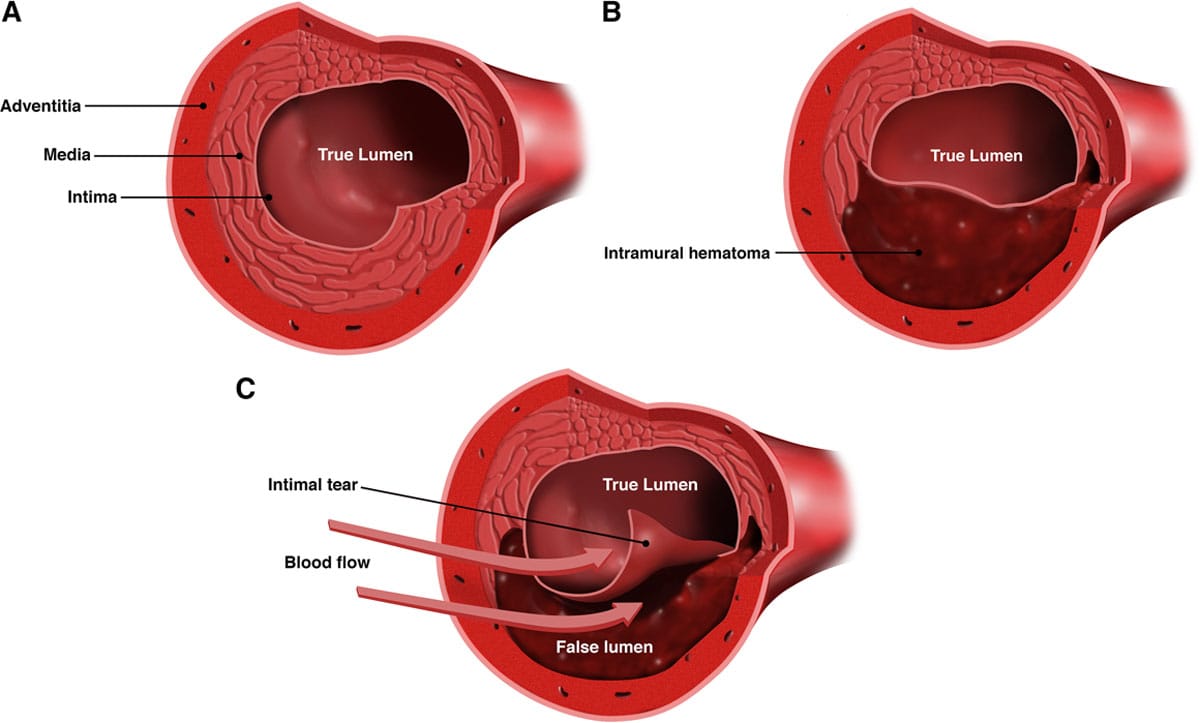
- The pathophysiology involves a spontaneous intramural thrombosis with or without an intimal tear. This obstructs the true lumen. The LAD is the most commonly affected but can occur in any artery.1
- Initial troponin can be normal but eventually most cases have elevated troponin. 1 Chest pain does not necessarily indicate myocardial ischaemia and can be a manifestation of the dissection itself. 1 From the urgent care perspective a normal POC troponin or an urgent lab troponin do not necessarily exclude the diagnosis.
- Coronary angiography is the investigation of choice and should occur asap as with STEMI.1 SCAD is an angiographic diagnosis of exclusion and so it is important to follow up these cases.2
- Management is controversial. An Open Evidence review suggests significant areas of uncertainty due to a lack of RCTs. Strategies include conservative management for stable low risk patients and PCI, CABG for high risk patients. Observational studies show high rates of spontaneous angiographic healing (70-90%) within weeks to months. There is a high recurrence rate.
- Complications- Early: ventricular arrhythmias, MI, cardiogenic shock, sudden death, recurrent dissection. Late: post-SCAD chest pain syndrome. 1
- Patient journey stories give us an interesting insight into the condition. 3
- The other aspects of this case relate to recognizing subtle hyperacute T waves (HATW) and understanding RV infarction.
- There is confusion and lack of knowledge about HATW. The attending paramedic crew in this case concerningly missed the significance of the initial ECG. There is still no universal definition of the appearance of a HATW but for some time now they have been known to be an early sign of occulsion MI (OMI). Perhaps they are so transient that they are often not seen. Compared to normal T waves, HATW are broader, more symmetrical, have more rounded peak/less concavity, and are larger relative to the QRS amplitude. They can be associated with reciprocal ST depression. The ECG below is very similar to the case described(I lost the original) caused by inferior OMI . Note the HATW in leads 3 and aVF.4,5
- The HATW topic is too large for this case report so I will return to this in a future dedicated post. The important point is that HATWs are a "STEMI equivalent" or sign of OMI and are an indication for emergency PCI.5,6
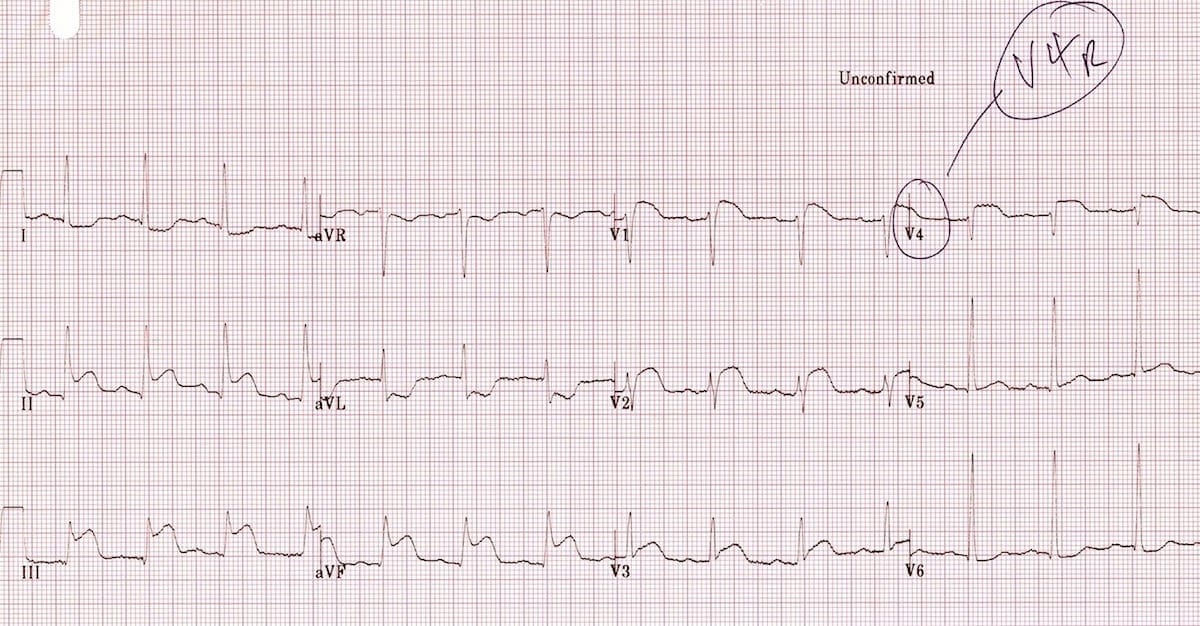
- The classic ECG changes in RV infarction:7
-ST elevation in V1- the only standard ECG lead that looks directly at the right ventricle
-ST elevation in V1 and ST depression in V2 (highly specific for RV infarction)
-ST elevation in III > II
-ST elevation in the right-sided leads (V3R-V6R) V4R diagnostic accuracy of 83% in the diagnosis of RV
- RV infarction complicates 40-50 % inferior STEMIs. Avoid nitrates/GTN with inferior MI. RV filling is preload sensitive.
- IV fentanyl for analgesia is probably best in view of the potential haemodynamic instability. Start with 20 mcg and titrate to response.
- Fluid-loading may be required for hypotension to optimise preload. An Open Evidence review for the optimal fluid in this situation suggests crystalloid eg plasmalyte 250-500ml boluses. In my general medical days we often gave the plasma expander Haemaccel but over the years this has generally lost favour in all types of resuscitation.
References
- Hayes SN, Kim ESH, Saw J, Adlam D, Arslanian-Engoren C, Economy KE, et al. Spontaneous coronary artery dissection: current state of the science: a scientific statement from the American Heart Association. Circulation [Internet]. 2018 May 8;137(19). Available from:https://www.ahajournals.org/doi/10.1161/CIR.0000000000000564
- Emergency Medicine Cases. Approach to Spontaneous Coronary Artery Dissection [Internet]. 2023. Available from:https://emergencymedicinecases.com/ecg-spontaneous-coronary-artery-dissection-scad/
- Heart Foundation NZ. Spontaneous coronary artery dissection (SCAD) [Internet]. Available from:https://www.heartfoundation.org.nz/your-heart/heart-conditions/spontaneous-coronary-artery-dissection
- Emergency Medicine Cases. Hyperacute T waves and Occlusion MI [Internet]. Available from:https://emergencymedicinecases.com/hyperacute-t-waves-occlusion-mi/
- Dr. Smith’s ECG Blog. Hyperacute T waves [Internet]. Available from:https://drsmithsecgblog.com/search/Hyperacute%20T%20waves/
- Buttner R, Cadogan M, Cadogan RB, Buttner M. OMI: replacing the STEMI misnomer. Life in the Fast Lane (LITFL) [Internet]. 2021. Available from:https://litfl.com/omi-replacing-the-stemi-misnomer/
- Burns E, Buttner R, Buttner EB, Burns R. Right ventricular infarction. Life in the Fast Lane (LITFL) [Internet]. 2018. Available from:https://litfl.com/right-ventricular-infarction-ecg-library/




