New Severe Headache
A case of cerebral venous thrombosis in a 55 year old man without risk factors. Discussion of clinical features, when to consider the diagnosis and current management.

A 55-year-old man arrived in urgent care with a history of a sudden, severe (10/10) headache, onset the night before. It was so bad that he had been unable to sleep. The next morning he attempted to go to work but became photophobic and vomited four times. He also mentioned possible diarrhoea, although this was vague. His overall history was difficult to follow, but he reported no fever, no past medical problems, and no regular medications.There was no past history of migraine. On arrival he looked unwell, leaning forward and holding his head, but he remained fully oriented.
On examination, his vital signs showed a blood pressure of 145/90 and a blood glucose level of 7.5 mmol/L. Neurologically he was lethargic but maintained a GCS of 15. He had mild photophobia but no neck stiffness, no rash, and no focal neurological deficits. His pupils were equal and reactive, his eye movements were intact, and there was no facial or limb weakness. Overall, he appeared clearly uncomfortable, but nothing on examination pointed to a definitive diagnosis.
My main concern with him was subarachnoid haemorrhage especially with the thunderclap nature of the headache. I thought the differentials included viral meningitis and migraine. There was clearly something not right with him and big red flag- age >50 with new onset headache. I referred him into the local Emergency Department for urgent CT Brain.
In the Emergency Department, a non-con CT/CT venogram revealed the diagnosis: extensive cerebral venous sinus thrombosis. The thrombosis involved the straight sinus, the left transverse sinus, the sigmoid sinus, and the proximal left internal cerebral vein. Routine blood tests were normal, and a thrombophilia screen—covering JAK2, PNH, Factor V Leiden, and Protein S—was also normal. He tested negative for COVID. CT abdomen and pelvis was also normal.
He was anticoagulated with clexane and later transitioned to dabigatran. His condition improved, and he was discharged after three days with planned follow-up by the haematology team.
Learning Nuggets
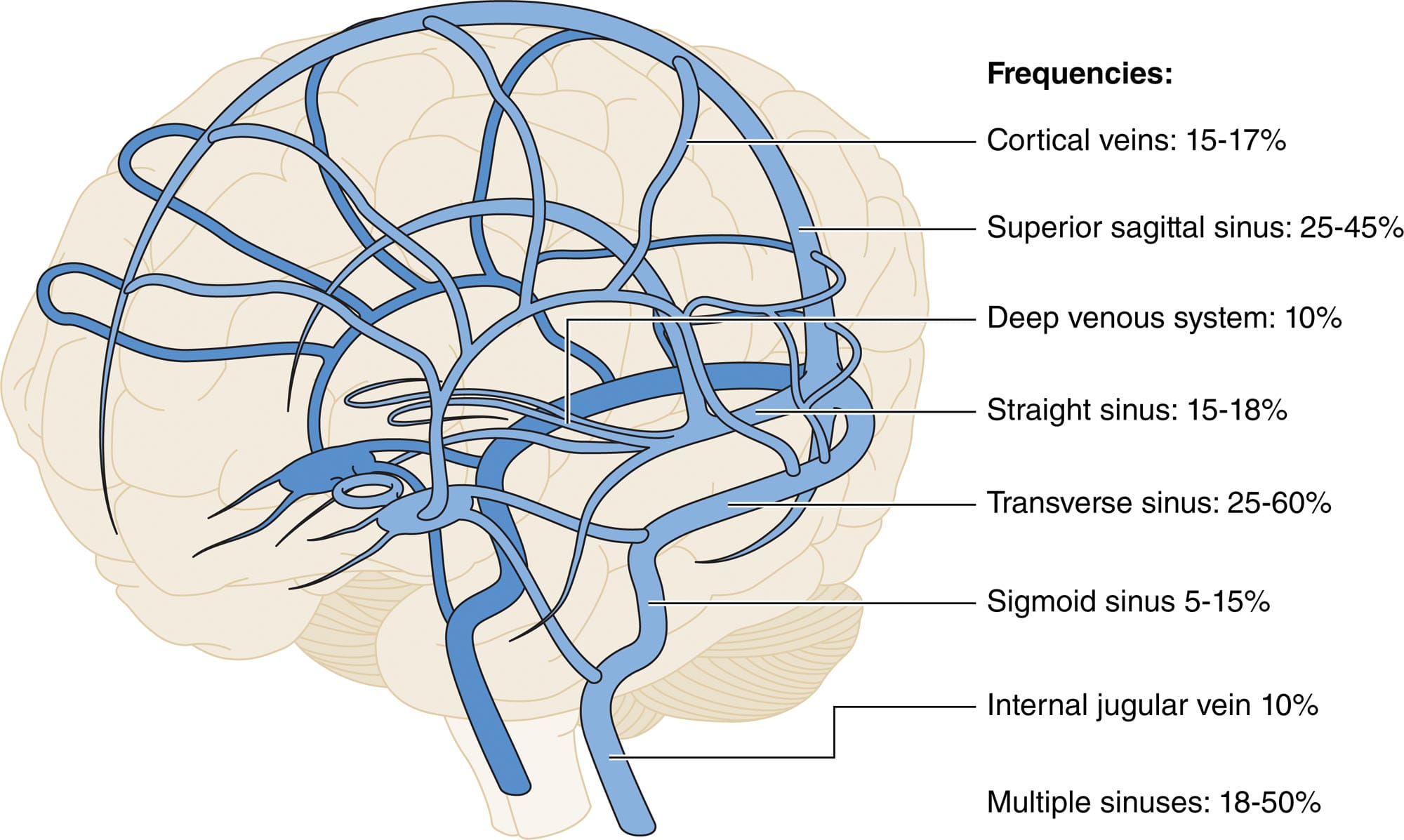
- Cerebral Venous Thrombosis (CVT) affects the dural venous sinuses, cerebral veins or both.
- CVT remains rare but under-recognized. It accounts for 0.5-3% of all strokes.
- Patient demographics and risk profiles are evolving. Mainly seen in the under 55 age group with 2/3 affecting women. Historically seen more in younger women (pregnancy, contraception), but newer data add risk factors such as obesity, COVID-19 and vaccine-induced thrombocytopenia to the list. Also not to be forgotten risk factors include head/neck infections, dehydration, sepsis, anaemia and meningioma and malignancy.
- Wide and often non-specific clinical presentation — vigilance is required. Headache remains the most common symptom(90%). Often insidious in onset: most present >48 hrs after onset. Acute presentation with thunderclap headache or SAH (<5%); acute focal neurological deficits (5-40%). Visual symptoms (13-27%). Papill0edema and diplopia (6%–14%). Seizures at the time of presentation(20-40%). Encephalopathy and coma (upto 20%).
- Don’t dismiss “just a headache” — especially in the presence of risk factors. Given the variable and sometimes non-focal presentation, CVT can be missed if only obvious “stroke-type” signs are considered.
- Be alert to combinations of symptoms — e.g., headache + new-onset seizure, headache worsening with Valsalva (cough/straining), signs of raised intracranial pressure (papilledema, visual blurring), or focal deficits not conforming to arterial territories. Such combinations should raise suspicion of venous causes.
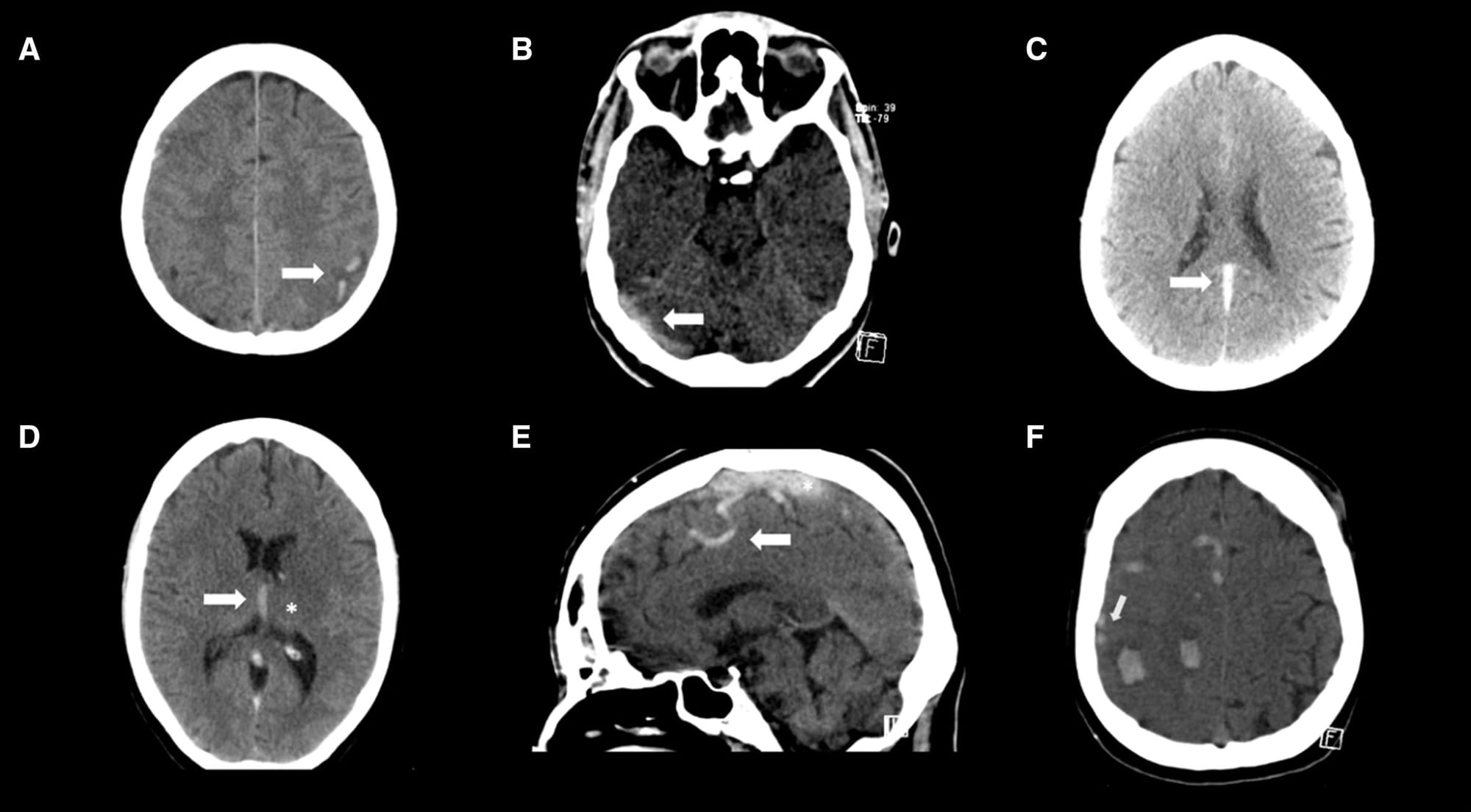
- Imaging: A normal non-contrast CT does not rule out the diagnosis of CVT. MR venography (MRV) or CT venography (CTV) are the optimal tests.
- D-dimer has no place in the acute investigation of CVT.
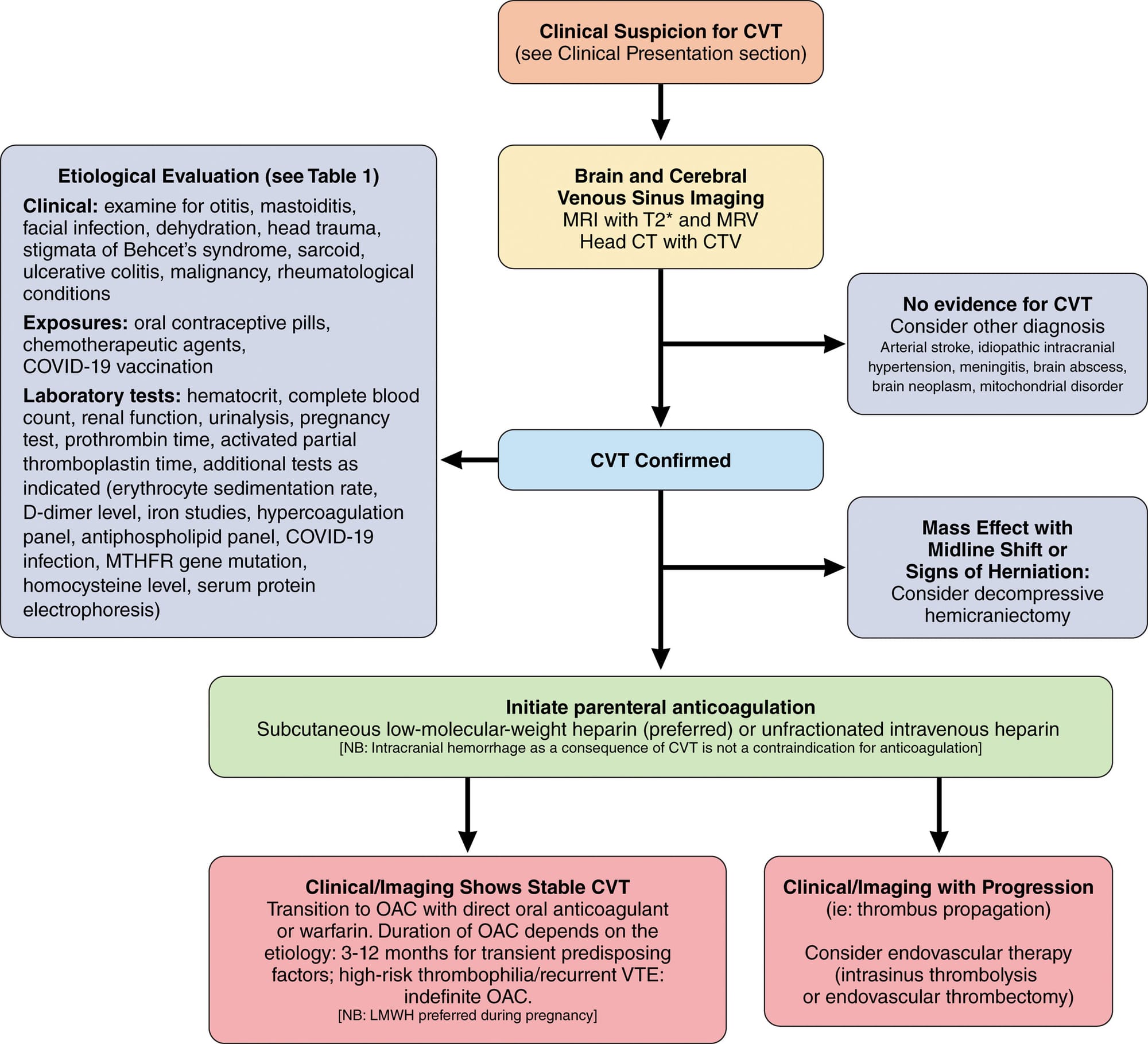
- Anticoagulation as the mainstay therapy in acute CVT and should be initiated asap.
- In selected cases, endovascular therapy (thrombectomy) or decompressive surgery may be considered.
- Plan follow-up and risk-factor evaluation before discharge. Given the range of underlying prothrombotic conditions (e.g. infection, thrombophilia, obesity, hormonal risk) and the possibility of long-term complications (headache, cognitive symptoms, recurrent thrombosis), ensure a pathway for further evaluation and long-term anticoagulation/monitoring as appropriate.
- Outcomes : 80% to 90% achieve functional independence/ epilepsy affects >10% / high prevalence of residual symptoms related to cognition, mood, fatigue, and headache.
Further Reading
- Saposnik G, Ferro JM, Canhão P, Coutinho JM, Stam J, Barinagarrementeria F, et al. Diagnosis and management of cerebral venous thrombosis: a statement for healthcare professionals. Stroke. 2023;54:e1–e14. Available from: https://www.ahajournals.org/doi/10.1161/STR.0000000000000456
- Gaillard F, Jones J, Weerakkody Y, et al. Dural venous sinus thrombosis. Radiopaedia. 2024. Available from: https://radiopaedia.org/articles/dural-venous-sinus-thrombosis




