Volar PIPJ dislocation
Case of a 65 year old man with a recurrent volar PIPJ dislocation. Discussion of anatomical considerations and management.

A 65-year-old man presented following an altercation on a golf course, during which he sustained a direct blow to his left ring finger from a golf club.

X-rays demonstrated a volar dislocation of the left ring finger PIP joint, with two small osseous fragments visible within the dorsal joint recess. The dislocation was easily reduced under a local anaesthetic ring block.

Post-reduction, the joint was clinically unstable and would re-dislocate with flexion of the PIP joint. The finger was immobilised in extension using a splint, and the patient was referred to hand therapy, with the instability noted in the referral. The report of the post reduction film suggested that there was a minor avulsion from the head of the proximal phalanx.
One week later, the patient re-presented with another volar dislocation of the same PIP joint. The hand therapist had replaced the original Zimmer splint with a thermoplastic splint. The patient reported striking his hand against a wall after waking suddenly. The dislocation was again reduced under ring block. Following this second reduction, the finger demonstrated a mild Boutonnière deformity. This time the radiology report suggested that the avulsion fragment was from the base of the middle phalanx.
Given the ongoing instability and concern for possible central slip rupture/avulsion, the patient was referred to the local Plastic Surgery team for further assessment and management. He underwent repair of the central slip with a bone anchor and K-wire with good result.
Learning Nuggets
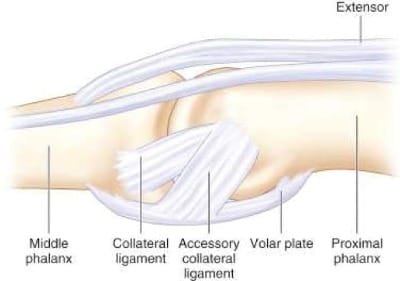
- Knowledge of the anatomy of the finger is key when assessing injuries. The PIPJ is stabilized by the collateral ligaments, the central extensor slip, FDS and the volar plate.1
- Volar PIPJ dislocations are much less common than dorsal dislocations but the true incidence is difficult to find. Some sources suggest they are rare.2,3
- Volar PIPJ dislocations are associated with central slip extensor tears/avulsions but again the true incidence is difficult to establish. Logic would tend to suggest that a central slip tear or avulsion is present in the majority of cases.
- There are different types of volar dislocations and different classification systems.2,3 In my view these are of limited use for the Urgent Care Physician. In simple terms there are broadly 3 types : 1) Central slip avulsion fractures, (2) Rotatory(pure dislocations)-due to rupture of one collateral ligament-and results in one of the proximal phalangeal condyles buttonholing between the central slip and lateral band, (3) Pilon fractures where there is a heavily comminuted fracture dislocation of the PIPJ.


- Reduction requires a different technique to dorsal PIPJ dislocations. The MCPJ should be flexed to relax the lateral bands then traction /manipulation of the middle phalanx is performed. Operative reduction is often required for rotatory dislocations which can be irreducible.1,3,4
- Post-reduction the stability of the joint should be assessed and Elson's test5,6 performed to assess the central slip extensor mechanism. Any Boutonniere deformity which can be subtle should also be noted.
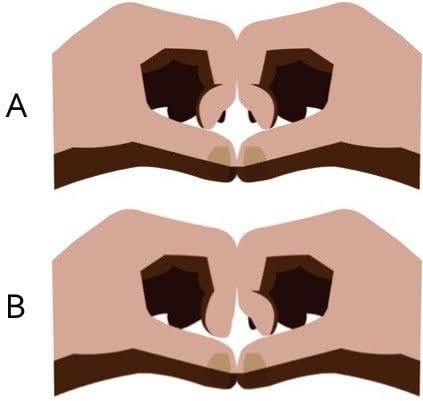
- In practice Elson's test is not always easy to perform or interpret. There is the traditional Elson's 5 and a modified version 6 which demonstrates the hyperextension of the DIPJ, as in in the left hand in (B).
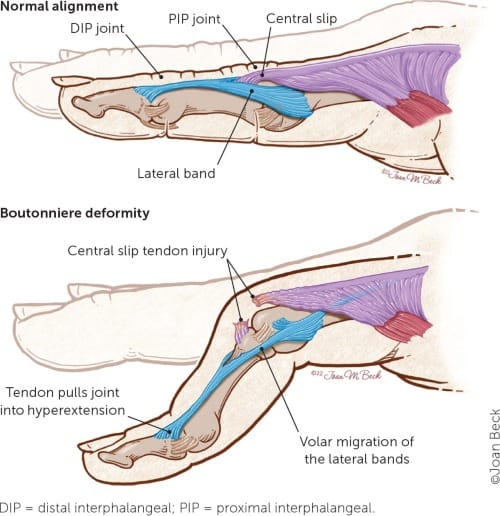
- A Boutonnière deformity is the main concerning complication of a central slip tear/avulsion fracture

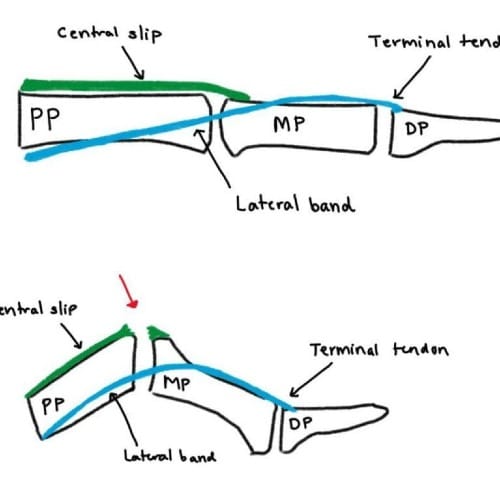
- The Boutonniere deformity sequence. (1) The PIP joint loses its dorsal extension force, so it starts to flex. (2) As the PIP flexes, the lateral bands slip volarly (below the axis of rotation of the PIP joint). (3) Once volar, the lateral bands act as flexors at the PIP joint rather than extensors—this locks in the deformity. Because the lateral bands are now tighter and pulled distally, they hyperextend the DIP joint. This results in flexion of the PIP joint with hyperextension of the DIP joint→ giving the characteristic “buttonhole” appearance — hence the name boutonnière (French for “buttonhole”).
- Advice on the post reduction management is confusing. Orthobullets suggests conservative management with splinting in extension for 6-8 weeks for simple volar dislocations.1 Non-surgical treatment is also suggested in some articles where there are small undisplaced dorsal lip fractures as in this case.3 "The primary aim is to re-establish central slip continuity to prevent a boutonnière deformity. Like a mallet fracture, the fracture can progress into osseous or stable fibrous union when properly immobilised".3 It seems that some volar dislocations can be treated conservatively but there are some complex factors to take into consideration here and this decision is probably best made by a hand surgeon.
- With the initial presentation of this patient my rationale for a trial of conservative treatment was that the avulsion fragment seemed very small. I noted the instability of the joint on my referral to the hand therapist. I referred to a hand therapy clinic which has a resident hand surgeon and I had expected that if there were any concerns the patient would have been referred internally to the hand surgeon.
- In summary volar PIPJ dislocations are rare and there are several complexities to management. Urgent care and ED physicians probably do not get enough exposure to these injuries. There is a high risk of central extensor slip injury but assessment for this is not always easy. Boutonniere deformity can develop.
- My advice- keep things simple. Reduce the dislocation. Document Elson's, instability and resting postion post reduction. Splint the joint in extension. Refer acutely to the local hand/plastics team.
References
- Phalanx dislocations - hand - Orthobullets [Internet]. Available from: https://www.orthobullets.com/hand/6038/phalanx-dislocations
- Jerome JTJ. Volar dislocation of the proximal interphalangeal joint. Orthoplastic Surgery [Internet]. 2021 Sep 1;5:6–8. Available from: https://www.sciencedirect.com/science/article/pii/S2666769X21000154
- Choke A, Tan RES, Cheah AEJ. A review on volar fracture–dislocations of the proximal interphalangeal joint. J Hand Surg Asian-Pac Vol [Internet]. 2024 Jun;29(03):163–70. Available from: https://www.researchgate.net/publication/380486181_A_Review_on_Volar_Fracture-Dislocations_of_the_Proximal_Interphalangeal_Joint
- Editor DT. Wheeless’ Textbook of Orthopaedics. 2020. Volar PIP dislocation. Available from: https://www.wheelessonline.com/muscles-tendons/volar-pip-dislocation/
- Quick clinical tip: Elson’s test for the finger [Internet]. Available from: https://www.aliem.com/elsons-test/
- Diagnosing central slip injury [Internet]. Available from: https://www.aliem.com/diagnosing-the-central-slip-injury/



